Medical imaging just ran into its first deepfake crisis. A new Radiology study shows that synthetic X-rays generated by multimodal AI are now indistinguishable from real scans for most radiologists and even other foundation models. That means anyone with access to a hospital archive—or a motivated fraudster—could inject fake fractures, fabricate injuries, or destabilize clinical workflows with a single malicious upload.
What the new study found
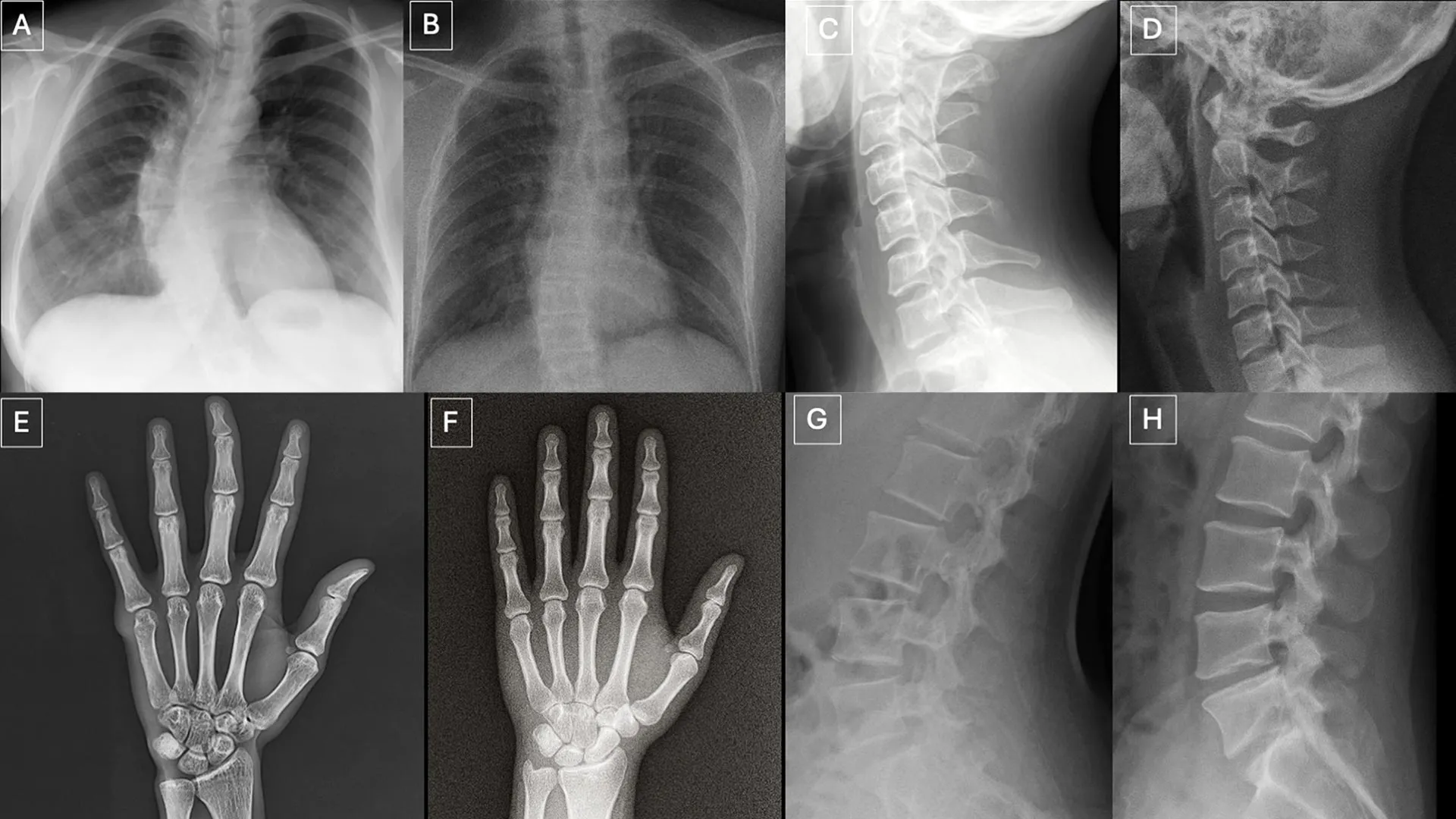
Researchers from Mount Sinai tested 17 radiologists across six countries on two datasets: one mixed set with GPT-4o–generated X-rays from multiple body parts, and another chest-only set created with Stanford’s RoentGen diffusion model. They then challenged four leading multimodal models (GPT-4o, GPT-5, Gemini 2.5 Pro, and Llama 4 Maverick) with the same images.
- Radiologists spotted GPT-4o deepfakes only 41% of the time when they didn’t know synthetics were included; accuracy rose to 75% when they were warned.
- Performance varied wildly: the best human reader hit 92%, the worst 58%. Experience level had no correlation with success.
- The AI judges didn’t fare better—accuracy ranged from 57% to 85%, meaning the models that generate imagery also struggle to police it.
- Synthetic images shared recognizable “tells”: unnaturally smooth bones, symmetrical lungs, perfectly aligned spines, and fractures that looked too clean or appeared only on one side of a limb.
The research team is already publishing an open deepfake dataset plus training quizzes, but they caution that CT and MRI are the logical next targets. If a 2D chest film can be forged this convincingly, volumetric scans are not far behind.
Why it matters beyond hospitals
This isn’t just a medical story; it’s the same authenticity problem every robotics and AI practitioner will face as synthetic data becomes routine. Consider three immediate spillovers:
- Litigation risk. Deepfake evidence could flood insurers and courts with “proof” of injuries that never happened, delaying legitimate claims and spiking compliance costs.
- Operational sabotage. A compromised PACS archive is enough to paralyze a hospital. The same attack vector applies to robotics labs that rely on shared datasets or remote teleoperation feeds.
- Model drift. Training perception systems on doctored data quietly poisons downstream robots, surgical assistants, or inspection pipelines.
Aswin’s take: build provenance in, not after the fact
Healthcare won’t solve this with better eyeballs alone. Provenance has to live at the point of capture, just like torque sensors live on a robot joint. My playbook for hospital partners (and frankly, any AI-heavy enterprise) looks like this:
- Cryptographic signatures on acquisition. Bind each image to the technologist, modality ID, and timestamp using tamper-proof signatures. This mirrors the chain-of-custody work we already do for industrial robots.
- Invisible watermarks baked into sensor firmware. If the imaging vendor embeds watermarks at the detector level, any alteration becomes obvious without extra hardware.
- Dual-model validation. Pair diagnostic AI with a lightweight discriminator trained solely to spot “too-perfect” anatomical cues. Treat it as a watchdog, not a primary reader.
- Red-team drills. Hospitals should run the same kind of adversarial exercises we use in robotics safety audits: inject synthetic files, watch how staff respond, and close the gaps.
Do that and you blunt both the legal exposure and the patient-safety risk before regulations catch up.
What to watch next
- Vendors like GE HealthCare, Siemens, and Philips rolling out signed-image pipelines.
- Multimodal watermarking standards that span X-ray, CT, MRI, ultrasound, and even robotics perception sensors.
- Insurers updating policy language to require provenance for high-value claims.
The headline is simple: synthetic imagery is now good enough to fool experts. If you’re building or buying AI systems that rely on visual data—whether in an operating room or a factory—you’ll need authenticity infrastructure as urgently as you need accuracy.
Source: “Deepfake X-rays are so real even doctors can’t tell the difference,” ScienceDaily, March 26, 2026.
